What nearly 500 experienced professionals revealed about the Mental Health Act, the Mental Capacity Act, and the decisions in between
21 May 2026
Over two webinars, nearly 500 professionals working across mental health, acute care, social care, local government, policing, safeguarding, legal services and independent provision came together to discuss a subject that, despite its importance, is rarely explored at this scale or across such a broad mix of professions: the operational intersection between the Mental Health Act and the Mental Capacity Act.
These were not passive observers or people with a general professional interest in mental health law. The majority were people whose day-to-day work places them directly inside the consequences of these frameworks.
Across the system, there is growing recognition that the relationship between the Mental Health Act and the Mental Capacity Act is no longer simply a legal question. It is an operational one, being felt every day by the professionals asked to make, support or later defend high-stakes decisions in environments defined by time pressure, incomplete information, stretched resources and shared risk.
The Mental Health Act has entered a period of staged reform. The Mental Capacity Act Code of Practice, first published in 2007, now sits against nearly two decades of case law, service redesign and changing models of care. Liberty Protection Safeguards remain unresolved. At the same time, rising demand, workforce shortages, reduced bed capacity and increasing reliance on non-specialist environments mean decisions that may once have sat within specialist teams are now being made across a much wider range of settings.
Against that backdrop, the purpose of the sessions was not simply to revisit the legal architecture of either Act. It was to examine what happens when professionals find themselves in situations where both frameworks appear relevant, where neither framework offers a clean operational route, or where the law may technically provide authority but the surrounding system makes implementation far less straightforward.
Where professionals say current guidance falls short
When attendees to a webinar series hosted by Thalamos and law firm Weightmans were asked where current Codes of Practice fall short in supporting real-world decision-making, the responses were revealing.
The strongest themes did not centre on technical legal definitions or abstract rights-based debates. Instead, they focused on the places where operational complexity makes legal application harder: fluctuating capacity, disagreement between professionals about which framework applies, uncertainty around objection, managing restrictions that may amount to deprivation of liberty, and knowing what needs to be recorded when decisions are later challenged.
Where does the Mental Health Act Code of Practice fall short in supporting real-world decision-making?
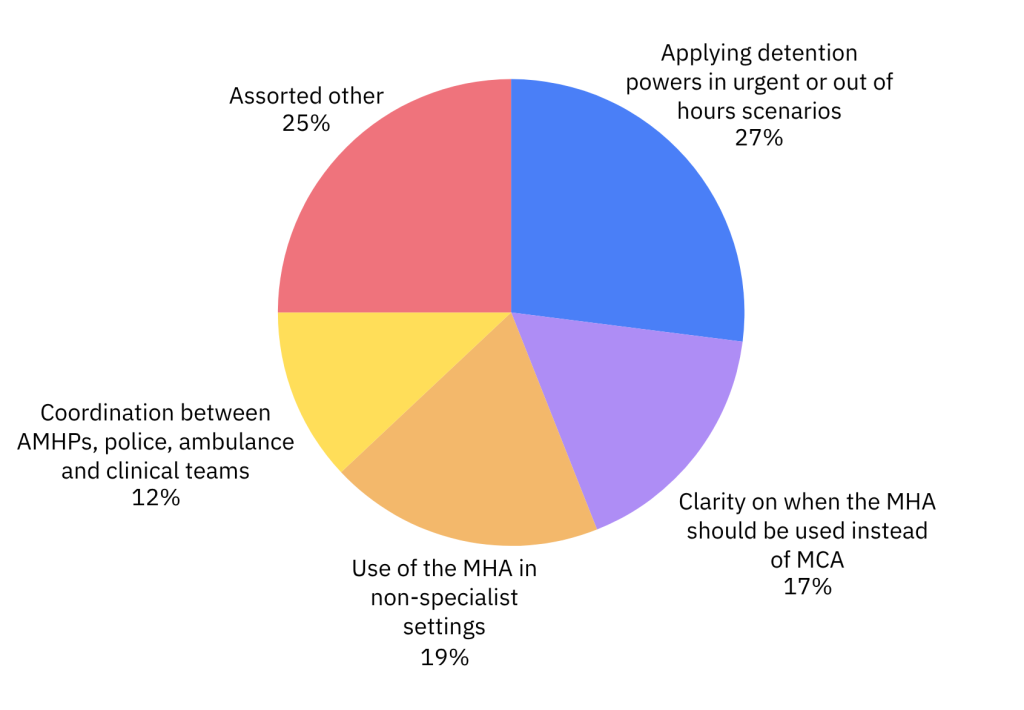
When participants were asked what should be prioritised in future revisions to the Mental Health Act Code of Practice, one theme stood out above the rest: clearer guidance on the interface between the Mental Health Act and the Mental Capacity Act.
That finding is difficult to ignore. Both Acts have been embedded in professional practice for years. Yet among those applying them most regularly, there remains a clear sense that the boundary between the two is still one of the least settled areas of frontline decision-making.
The Mental Capacity Act brings a different kind of uncertainty
When the same questions were asked about the Mental Capacity Act, the pattern shifted slightly.
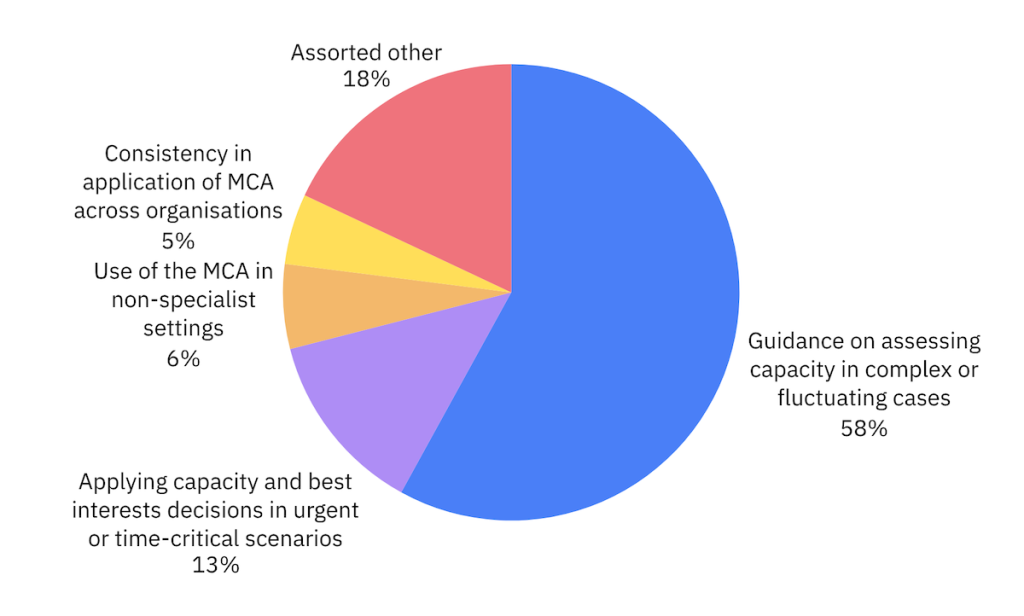
Here, uncertainty focused less on choosing between frameworks, and more on the complexity of capacity-based decision-making itself. Professionals repeatedly highlighted fluctuating capacity, best interest decision-making, deprivation of liberty, and the challenge of recording decisions made across multidisciplinary teams, often in settings never designed around legal workflow.
Where does the Mental Capacity Act Code of Practice fall short in supporting real-world decision-making?
This is perhaps unsurprising as capacity-based decisions are now being made not just in specialist mental health environments, but in emergency departments, general wards, ambulances, care homes, community services and social care settings, often without immediate access to specialist legal advice in the moment.
That flexibility is one of the strengths of the Mental Capacity Act. But it also creates a different kind of challenge. When decisions are made across settings, across teams, and often under significant pressure, they can become harder to evidence, harder to escalate, and harder to reconstruct later.
Confidence in current guidance remains cautious
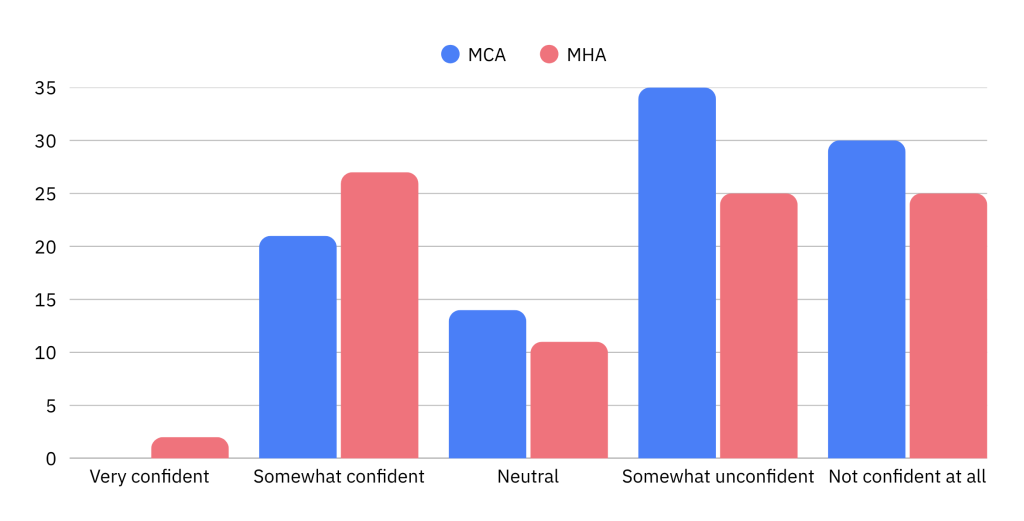
When attendees were asked how confident they were that current Codes of Practice reflect the realities of frontline decision-making, the results told their own story.
Very few respondents selected the highest levels of confidence. Most sat somewhere between “somewhat confident” and “somewhat unconfident.”
How confident are you that current MHA and MCA Codes of Practice reflect frontline realities?
This distinction matters. It suggests the challenge is not necessarily a lack of legal knowledge. It may be that the environments in which these decisions now take place have evolved faster than the systems, processes and guidance supporting them.
The questions behind the legislation
The live questions submitted during both sessions brought that reality into sharper focus.
Professionals described scenarios involving patients who appeared to meet Mental Health Act criteria, but where doctors and approved mental health professionals disagreed on the most appropriate route. Others described fluctuating capacity over the course of a single shift, uncertainty about whether restrictions in acute settings amounted to deprivation of liberty, or situations where the legal framework appeared clear, but no bed, service or escalation route was practically available.
Across all of these scenarios, a consistent pattern emerged. The challenge was rarely framed as not knowing the law. More often, the challenge was operational.
How does information move between professionals at speed? How do teams escalate disagreement? What happens when one organisation believes one framework applies and another does not? How do professionals document decisions under pressure? And when those decisions are reviewed months later, can anyone still clearly understand what happened, what alternatives were considered, and why a particular route was taken?
When scrutiny comes, what actually gets examined?
One of the strongest themes to emerge across both sessions was that when difficult decisions are later scrutinised, the first questions are rarely about whether professionals knew the legislation.
More often, scrutiny begins somewhere far more operational.
- What information was available at the time?
- Who contributed to the decision?
- What alternatives were considered?
- What escalation took place?
- What risks were identified?
- And can the reasoning still be clearly understood once the immediate pressure of the moment has passed?
That distinction appeared to resonate strongly with the audience, particularly given how many attendees were working in environments where responsibility for a person often moves across multiple organisations in the space of hours.
The legislation may provide authority. But professionals still need systems around them that provide visibility, chronology, accountability and confidence.
What this may tell us about the future
One of the more interesting discussions across the second session centred on how the Mental Health Act world has spent much of the last decade moving away from paper records, fragmented handovers and organisation-specific workflows towards more structured, auditable and cross-organisational approaches to decision-making.
What happens when an area of practice recognises that legal compliance alone is not enough, and that the ability to evidence decisions across organisational boundaries becomes just as important as the decision itself?
For many attendees, the obvious question was whether capacity-based decision-making may now be approaching a similar moment.
Not because the Mental Capacity Act should mirror the Mental Health Act, but because many of the underlying pressures are beginning to look increasingly familiar.
What nearly 500 professionals told us
If there was a single message that emerged from bringing this many professionals into one conversation, it was not that the sector lacks expertise.
It was that many of the people closest to these decisions increasingly feel that the frameworks around them have not evolved at the same pace as the environments in which those decisions now take place.
As Mental Health Act reform progresses, and as capacity-based decision-making becomes more central to urgent and emergency care pathways, that gap is likely to become harder to ignore.
If you want access to future events, expert briefings and conversations like this, subscribe to hear from Thalamos and be part of what comes next.
Stay up to date with insights like this one by following Thalamos on LinkedIn or joining our mailing list.


