Our impact
Our solutions improve the efficiency, accuracy, and overall patient care.
A unified, interoperable, and fully digital mental health crisis care pathway that has revolutionised patient care in the UK.
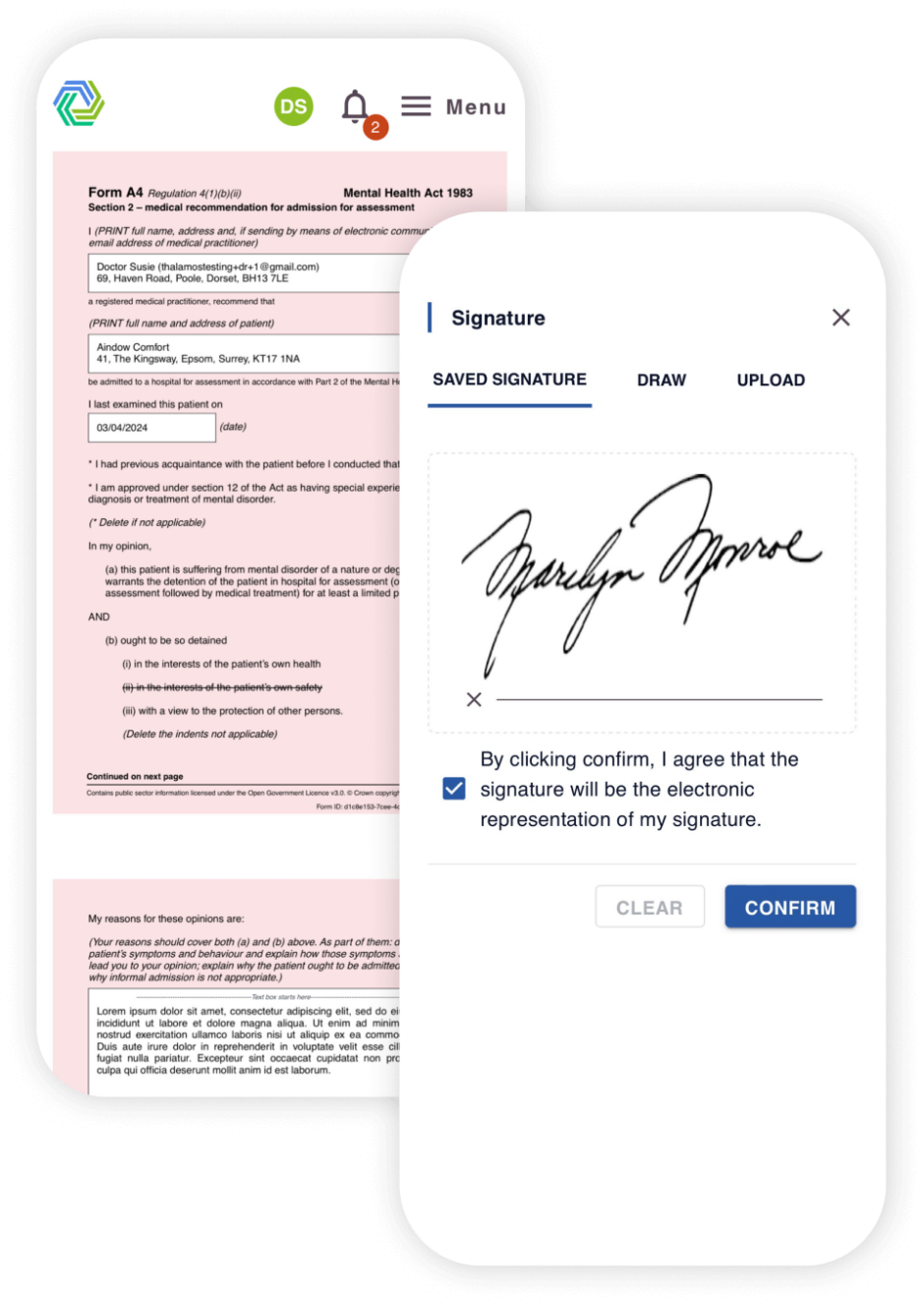
Providing secure completion and communication of Mental Health Act statutory forms, on any internet connected device, that are then shared digitally with all clinical & statutory stakeholders involved in the care pathway.
Thalamos reduces inefficiencies, improves patient care, and supports better health outcomes.

The fundamental objective of MHA Digitisation is to improve patient outcomes, speed up recovery, and deliver a better patient experience whilst in care. By treating patients in the shortest time possible they can be discharged from hospital much quicker.

Thalamos allows multiple agencies and care providers (Hospitals, Police, Social Care, CQC) to seamlessly communicate, interoperate, and fulfil statutory roles within the Mental Health Act whilst providing mental health crisis care.

By digitising the existing paper based system and care pathway Thalamos has reduced typical clerical errors on MHA forms by 90%, significantly speeding up treatment times.

Time to treatment has reduced from upwards of 14 days to less than 24 hours so patients receive the care they need without delay. Time savings are redeployed into wider patient care focusing extra resources on reducing waiting lists and maximising existing budgets.

By improving inter agency communication, we isolate both high and operational level data insights creating visibility across key performance metrics that were previously unachievable.

By removing administrative burden, we allow staff across the mental health act pathways and different organisations to focus on patient care and remove the unnecessary time spent on administrative tasks.

Thalamos technology enables all system wide care providers involved in the mental health care pathway to communicate and interoperate digitally.

Thalamos eMHA software enables mental health hospital trusts to manage the end-to-end Mental Health care pathway more efficiently than with existing paper-based systems.

Thalamos supports Social Services and AMHPs, who are responsible for admitting patients to hospital, to complete their statutory roles more effectively so patients receive treatment without delay.

Thalamos enables Private care providers to manage the end-to-end mental health care pathway across all their geographic sites, delivering true oversight of MHA clinical performance.

Thalamos works with the Metropolitan Police Service across London to manage the entire Section 136 care pathway, meaning patients are taken to the nearest available place of safety more quickly.

Thalamos is the sole provider of digital Second Opinion Appointed Doctor forms and processes to the Care Quality Commission. 95% of Mental Health Trusts have received SOAD forms from Thalamos.
We believe that there should be no distinction or disparity between emergency physical and mental health care as exists currently.
Our solutions improve the efficiency, accuracy, and overall patient care.
Thalamos has helped reduce access to treatment times from 7 days to 15 hours.

Patients can be discharged 1-3 days sooner by trusts using Thalamos.

At one site using paper, there was an estimated 25% error rate, this error rate has been dramatically reduced to 1.6% since using Thalamos.














When a close friend of Arden’s was sectioned under the Mental Health Act, there was disbelief that an emergency care pathway was managed by moving around paper forms.
Disbelief turned to shock when it became apparent that access to treatment would be delayed whilst they waited for the set of forms to be circulated manually and finally signed off.
Thinking there must be a quicker and more efficient way of accessing treatment during a mental health crisis, Arden and Ross founded Thalamos to digitise the entire care pathway.
Existing customers
If you are looking for support while using Thalamos, please email support@thalamos.co.uk or call 0203 886 0385.
If you work for, or with: